Birth Control to the Rescue? How Oral Contraceptives REALLY Impact An Athlete
By Emily R Pappas, MS
For many female athletes, experiencing an irregular or missing period during the sport season seems “normal”. In an attempt to “bring her period back”, some doctors may still suggest taking an oral contraceptive.
But for many female athletes, an irregular cycle is a signal that a female athlete’s natural hormones are not working properly. Placing a young adolescent female on an oral contraceptive may create an illusion that her period is “regular”, BUT it does NOT mean that her hormones are working optimally.
Unfortunately, current research shows us taking an oral contraceptive is a “band aid” to the problem and does not address the CAUSE.
For female athletes considering taking an oral contraceptive for irregular or missing periods, this article is a MUST to learn:
What an irregular, missing, or painful cycle could be signaling
How hormones are related to BONE HEALTH & INJURY RISKS
How oral contraceptives affect the female athlete’s natural cycling hormones
What the current research says about prescribing oral contraceptives to adolescent female athletes
The Danger of Missing Periods
“I’ll do just about anything to make sure I get my period. I’ll eat an entire jar of peanut butter if I have to!”
That’s a quote from ironman champion and triathlete Meredith Kessler.
Meredith has always loved running. At 14, she would run up to ten miles before school everyday. Her passion for sports continued into high school where she became a four-sport athlete in track, field hockey, swimming, and lacrosse.
But at the age of 19…something was wrong.

Meredith hadn’t had her first period.
Now we know this should have been a BIG RED FLAG. In The Danger of RED-S, we talked about how absent or unpredictable periods mean your body is being under-fueled.
But Meredith’s doctor did what most medical professionals do: prescribed oral birth control.
Girls, it’s time we talk about it. Period issues like missed periods or abnormal cycles are a SIGNAL.
Taking an oral contraceptive for period regulation is a BANDAID- NOT a solution.
Oral Birth Control: Quick Fix For A Long Term Problem

Fresh from High School, Meredith discovered she had borderline osteoporosis.
“I had borderline osteoporosis because I wasn’t getting those regular doses of estrogen,” she explained. “I was breaking things so easily…I remember how devastated I was when I broke my hip while competing and my dad had to carry me off the track.”
The bottom line is that female athletes who sustain high training loads are more likely to see changes in the menstrual cycle. These changes, like oligomenorrhea (irregular cycles) and amenorrhea (complete absence) mean BIG RISKS to the female athlete’s long term health.
There are many things to consider when it comes down to menstrual cycle changes (like polycystic ovarian syndrome, chronic disease, and pregnancy). But for the female athlete, research shows us, most of the time, it comes down to an imbalance of STRESS on her body (from training, competition, school, family, etc.), coupled with inadequate recovery (lack of sleep, lack of downtime, low energy intake, etc.).
Why?
Her body is trying to SURVIVE.
When stress levels never let up, the female athlete’s ability to recover diminishes. When this happens, her body’s natural survival instincts kick in.
Anything her body doesn’t deem “vital” for survival doesn’t get the energy it needs to function…and one of these systems, you guessed it, is her reproductive system. (3)
If your athlete is not trying to get pregnant, this might not look like a problem….
But it IS a problem.
The female athlete’s body is an INTEGRATED system. It doesn’t just use hormones like estrogen for making babies. Hormonal trouble can lead to gastrointestinal problems, cardiovascular risks, bone health, injury risks, and, most important to the female athlete, the longevity of her athletic career… (5).
We broke down the science behind how each hormone affects your body’s function in this article.
Then we talked about how to leverage your menstrual cycle to train at your best.
Now, we want to dive into the practice of taking oral contraceptives to “fix” period problems. And how OCPs can put the female athlete’s performance- and health- at risk.
Bones 101: The relationship between HORMONES & BONES
“Amenorrhea is also linked to a reduction in the body’s capacity to absorb calcium, decreases bone density and increases the risk of musculoskeletal injury.” (8)
During puberty, the body starts accumulating bone mass, reaching its peak around the age of 26 for females.
Ok, but what does this have to do with missing a period?
Estrogen, the “main” hormone the female athlete’s body produces during a normal cycle, does more than help your ovaries mature an egg.
It also affects injury recovery, muscle regeneration, and BONE FORMATION (10,11).

The Life Cycle of A Bone
Did you know all bones have a “life cycle” too?
Mature bone tissue is continuously broken down and reabsorbed by the body and new bone tissue is formed to take its place. This happens throughout an athlete’s entire life. The building cycle is called Bone Formation, and the breaking down is called Ossification.
The female athlete’s bones are broken down by cells called Osteoclasts.
Estrogen has a unique impact on osteoclast cells. It slows their activity down enough that the body is able to not only rebuild but increase formation and mineralization. (4). This allows for a faster recovery time!
During puberty, estrogen, coupled with growth hormones and insulin-like growth factors, give the body a tremendous boost in the bone-building process. Estrogen also drives the end of puberty where the epiphyseal opening of the bones is closed.
When this happens, the female athlete’s body is pretty much done creating bone mass. 90-99% of lifetime bone mass has been built by the age of 26 (2). Post-puberty, healthy women with good estrogen levels balance ossification and bone formation, maintaining this bone density through adulthood.
You see, female athletes shouldn’t have to worry about things like osteoporosis until after menopause… when the loss of estrogen during menopause throws this balance off.
Low density bones mean high risk of injury.
For female athletes who experience an irregular or missing cycle, this is a SIGNAL that hormone levels including estrogen are off, thus decreasing the female athlete’s ability to build strong & dense bones!! (10).
The fact that high-school aged female athletes are seeing signs of osteoporosis before they’re 20 means that something is seriously wrong!

How Bone Mass Gives Females A Lifetime Advantage
When a female athlete mixes sports training with puberty…she stresses her body to build STRONG BONES. With the right amount of fuel for recovery, she provides her body with the building blocks she needs to respond to this training and develop a strong basis of bone & muscle mass!
Studies show that adolescent females who participate in competitive sports and strength training have a HIGHER BONE MINERAL DENSITY in adulthood than those who don’t (9).
But…here’s the catch:
She ONLY gets this advantage if her body has the right hormonal environment that enables bone mass accrual…..
This means:
Getting Enough Fuel to maintain good energy balance
If the female athlete’s period is missing or irregular, she is NOT producing the estrogen she needs to accrue this bone mass.
This means a high risk of injury now…and throughout her entire career! (5)
ORAL CONTRACEPTIVES TO THE RESCUE……OR ARE THEY?
At 26 years old, Meredith Kessler decided to ditch the oral contraceptives and make a commitment to solving what was really holding her performance back: under-fueling.
Was the doctor wrong to prescribe them to her in the first place?
Prescribing oral contraceptives to female athletes WAS a common way to address period problems.

Cognitively, it makes sense why the oral contraceptive pill (OCP) containing estrogen and progestin should help those suffering from amenorrhea….
If the female’s body does not have enough estrogen to promote recovery & bone growth,
The problem? Studies on OCP’s effects on bone mineral density is not only INCONCLUSIVE (3) but also have demonstrated a DECREASE in bone mineral density when administered to athletes during this pubescent period (11).
Why?
Consider this:
When athletes take an OCP they are putting what is called an “exogenous synthetic hormone” into their body.
When the body gets an outside hormone, it stops making its own.
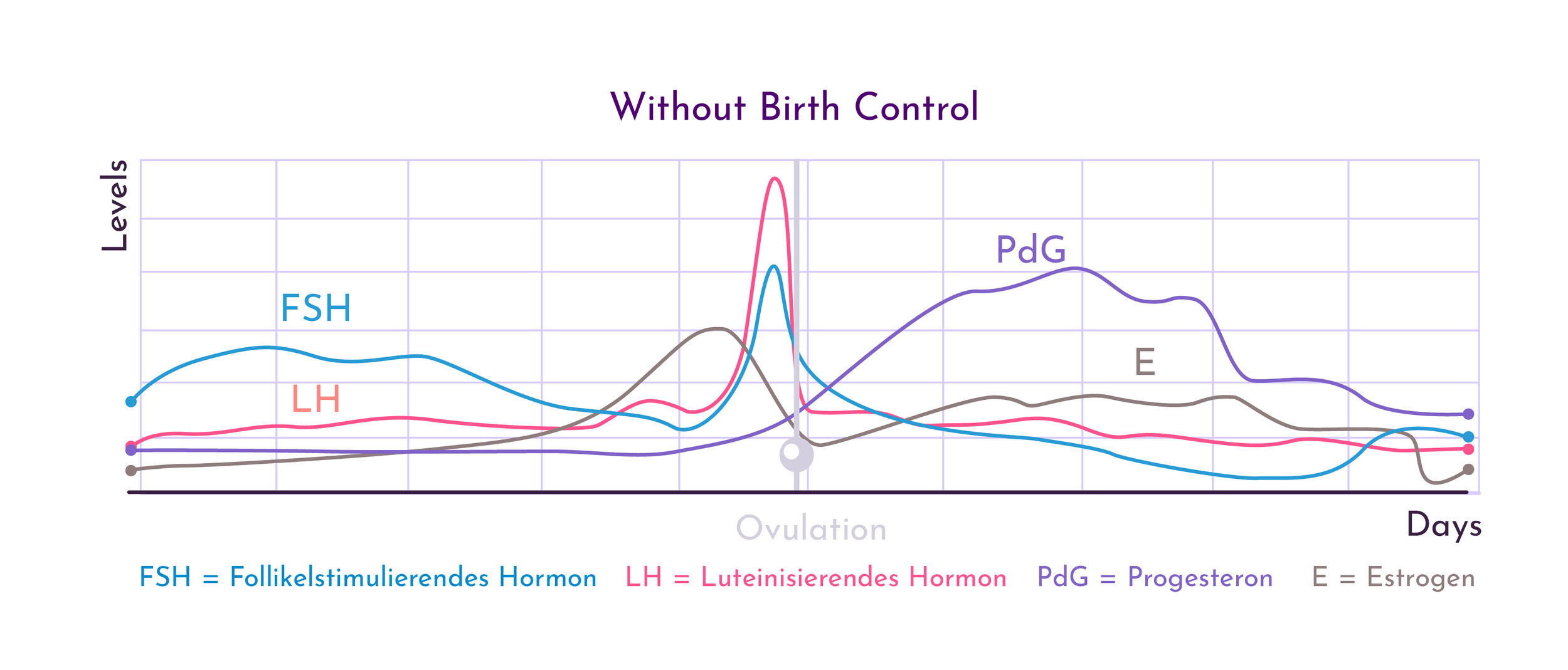
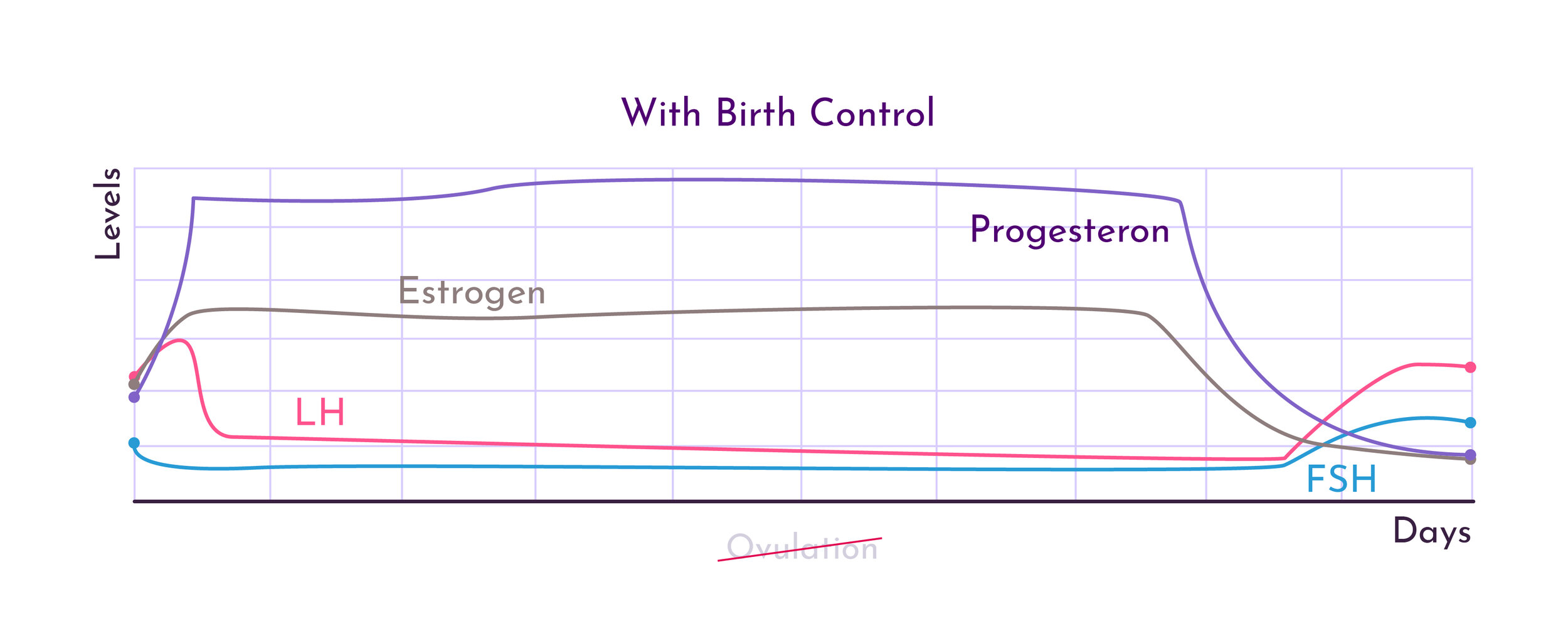
To get technical, the OCP systemically controls concentrations of endogenous sex hormones by reducing the female athlete’s natural production of estrogen and progesterone via the inhibition of the hypothalamus-pituitary-gonad axis (5).
Basically, the OCP provides the female athlete’s body with hormones to make it think it is “pregnant”. This in turn, inhibits ovulation…so there isn’t any egg available to fertilize.

“But I have a normal period when I am on the pill!!”
NOT REALLY.
The “period” that the female athlete gets while on the pill isn’t a real period.
You see, having a period is a signal (although not 100% accurate), that the female athlete has OVULATED! When the uterus does not get implanted with a fertilized egg, the lining is shed and the female athlete bleeds! All a signal that her hormones are cycling the way they should!
But on the pill, ovulation DOES NOT HAPPEN. And the female athlete’s natural hormones are NOT cycling the way they would without the pill.
The “period” an athlete experiences on a pill is NOT A PERIOD, rather, it’s a withdrawal symptom from the lack of hormones her body is getting during the blank pill week!
Now…just to be clear….there are MANY OCPs out there that differ in hormone type (estrogen only, PROGESTIN* only, combo pills) as well as hormone fluctuations (monophasic, biphasic, triphasic).
Unfortunately, modern science has not performed enough research on the different type of SYNTHETIC hormones in these pills as well as the different fluctuating pill types! (Yup even in 2020 we still do not know how all of these hormones actually affect our bodies long term….)
But what we do know is that OCPs are an EXOGENOUS HORMONE that STOPS OVULATION in the short term.

Ok, but when not on a pill, what does missing a period mean for an athlete?
If a female athlete is missing her period…9 times out of 10 this means she is NOT OVULATING.
If the body is not doing something it should be doing…don’t you think the first questions we SHOULD be asking is “WHY?”……
Taking an OCP to “just put the hormones back in the system” doesn’t fix WHY the problem is happening in the first place.
Even worse, OCP drastically decreases the production of the female athlete’s natural hormones completely. (2)
For a growing adolescent, this could be disastrous to her long term health….
Think of it this way: would you give a young adolescent boy testosterone if he wasn’t growing like his friends?
So why should a female athlete take an oral contraceptive to “regulate” her period???

Remember, the body is an INTEGRATED SYSTEM. Even when we consider just estrogen, we know it has an effect not just on the reproductive system, but also your bone health, your metabolism, and your energy levels (3).
In fact, estrogen has anti-inflammatory effects helping promote tissue recovery & muscle regeneration (10). With limited estrogen cycling in the body, not only in the reproductive system impacted, but also the female athlete’s ability to recover from tissue breakdown and sports training (3).
When an athlete takes an exogenous hormone (such as through an OCP), it essentially stops her natural production of that hormone.
When an adolescent athlete takes an oral contraceptive, she is tampering with more than just her period….
When considering bone health, it would make sense why doctors PREVIOUSLY believed the OCP would help females who are missing their periods receive the estrogen needed to inhibit osteoclast activity & promote bone accrual….
HERE’S THE THING: the estrogen in an OCP is not the same as the estrogen her gonads & adrenals produce.
That means it’s very possible that exogenous or outside hormones don’t work the same in this bone growth process. In a study performed by Nazem and colleges, athletes suffering from the female athlete triad who were provided with oral estrogen showed a DECREASE in systemic IGF-1 (an essential bone remodeling hormone) and therefore had NO benefit on bone health (6) .
Even if oral contraceptives did help bone mineral density, if an athlete is missing her period due to RED-S (i.e. she doesn’t have enough fuel), she’s also missing the energy and nutrients she needs for bone formation in the first place. (more on that HERE)
Taking an OCP because an athlete is missing her period doesn’t address the actual CAUSE of the missing period.
The LONG TERM consequences of taking an OCP during the pubescent period
A long term study in 1995 demonstrated athletes on OCP for 5 years showed a decreased peak BMD (bone mineral density) when compared to non-OCP counterparts (8).
Another more recent study in 2001 showed that those athletes taking OCP and following a resistance training protocol had a DECREASE in peak bone mineral density compared to non-OCP counterparts participating in resistance training (10).
Now these studies could indicate the OCP itself is inhibiting bone mass accrual…. OR they could indicate the OCP is not ADDRESSING THE PROBLEM at hand.
Although EVERY athlete is different, it is important to understand regardless of the positive or negative effects on bone health, OCPs are just a BANDAGE for the larger concern of females missing their menstrual cycle.
If a female athlete is not fueling her body to meet the demands of her SPORT & growing body, she does not have the energy she needs to promote bone accrual (ON or NOT on an OCP)….. (5,6,9).
A WORD ON OCPs For OTHER REASONS Beyond Irregular Menstrual Cycles
Just to be clear: this article is NOT against birth control.
Maybe female athlete has a regular cycle, but she has other physical issues like extreme cramps, a heavy flow, or acne….. Maybe determining the right balance of Omega 6: Omega 3 is worth considering (5). Or maybe taking an OCP is the next best step for HER!
For sexually active females, maybe OCP is the easiest choice for personal sexual wellbeing.
When it comes down to it, this is completely up to an athlete and her doctor.!
This article’s goal is to help athletes consider addressing the CAUSE of the problems.

At the end of the day, an athlete should NEVER, NEVER, never ever go to doctor and hide the fact that her cycles aren’t regular or that they’ve stopped. And, she must make sure to tell her gynecologist about her level of training & fuel intake!
Remember hormones affect one another. And reducing the production of an athlete’s own hormones CAN and WILL have effects on her other hormones both NOW and in the future.
So before jumping on the OCP train, make sure the female athlete considers the risk to reward ratio.
If taking the pill is the best way for her to handle other decisions or physical issues, then definitely consider it!
But if an athlete is considering OCP to regulate a missing or infrequent menstruation, it is essential she addresses to the root of the problem!
REFERENCES
(1)Burrows, Melonie, and Charlotte E Peters. “The Influence of Oral Contraceptives on Athletic Performance in Female Athletes.” Sports Medicine, vol. 37, no. 7, 2007, pp. 557–574., doi:10.2165/00007256-200737070-00001.
(2)Cromer, Barbara A. “Menstrual Cycle and Bone Health in Adolescents.” Annals of the New York Academy of Sciences, vol. 1135, no. 1, 2008, pp. 196–203., doi:10.1196/annals.1429.032.
(3) Eguiguren, Maria L, and Kathryn E Ackerman. “The Female Athlete Triad.” YOUNG FEMALE ATHLETE, SPRINGER, 2018, pp. 57–68.
(4)Hadjidakis, DJ, and II Androulakis . “Bone Remodeling.” Ann N Y Acad Sci., vol. 1092, 2006, pp. 385–396., doi:10.1007/springerreference_307955.
(5) Korsten-Reck, U. (2016, 03). The IOC Consensus Statement: Beyond the Female Athlete Triad – Relative Energy Deficiency in Sports (RED-S). Deutsche Zeitschrift Für Sportmedizin, 2016(03), 68-71. doi:10.5960/dzsm.2016.222
(6) Nazem TG, Ackerman KE. The female athlete triad. Sports Health. 2012; (4): 304-11
(7) Office of the Surgeon General (US). Bone Health and Osteoporosis: A Report of the Surgeon General. Rockville (MD): Office of the Surgeon General (US); 2004. 6, Determinants of Bone Health. Available from: https://www.ncbi.nlm.nih.gov/books/NBK45503/
(8) Polatti, Franco, et al. “Bone Mass and Long-Term Monophasic Oral Contraceptive Treatment in Young Women.” Contraception, vol. 51, no. 4, 1995, pp. 221–224., doi:10.1016/0010-7824(95)00036-a.
(9) Stracciolini, Andrea, et al. “Resistance Training for Young Female Athletes .” YOUNG FEMALE ATHLETE, SPRINGER, 2018, pp. 29–41.
(10) Tiidus P, Holden D, Bombardier E, Zajchowski, Enns D, Belcastro A. Estrogen effect on post-exercise skeletal muscle neutraphil in filtration and calpain activity. Can J Physiol Pharmacol 2001; 79: 400-406.
(11) Weaver, Connie M., et al. “Impact of Exercise on Bone Health and Contraindication of Oral Contraceptive Use in Young Women.” Medicine and Science in Sports and Exercise, vol. 33, no. 6, 2001, pp. 873–880., doi:10.1097/00005768-200106000-00004.
About the Author

Emily holds a M.S. in Exercise Physiology from Temple University and a B.S. in Biological Sciences from Drexel University. Through this education, Emily values her ability to coach athletes with a perspective that is grounded in biomechanics and human physiology. Outside of the classroom, Emily has experience coaching and programming at the Division I Collegiate Level working as an assistant strength coach for an internship with Temple University’s Women’s Rugby team.
In addition, Emily holds her USAW Sport Performance certification and values her ability to coach athletes using “Olympic” Weightlifting. Emily is extremely passionate about the sport of Weightlifting, not only for the competitive nature of the sport, but also for the application of the lifts as a tool in the strength field. Through these lifts, Emily has been able to develop athletes that range from grade school athletes to nationally ranked athletes in sports such as lacrosse, field hockey, and weightlifting.
Emily is also an adjunct at Temple University, instructing a course on the development of female athletes.